
When it comes to managing depression, Trazodone is a serotonin modulator and antagonist that’s also prescribed as a sleep aid. It was first approved by the FDA in 1981 and has been a go‑to option for patients who can’t tolerate classic SSRIs. This guide walks through how trazodone works, when it’s worth choosing, how to dose it safely, and what to expect in terms of benefits and side effects.
How Trazodone Works in the Brain
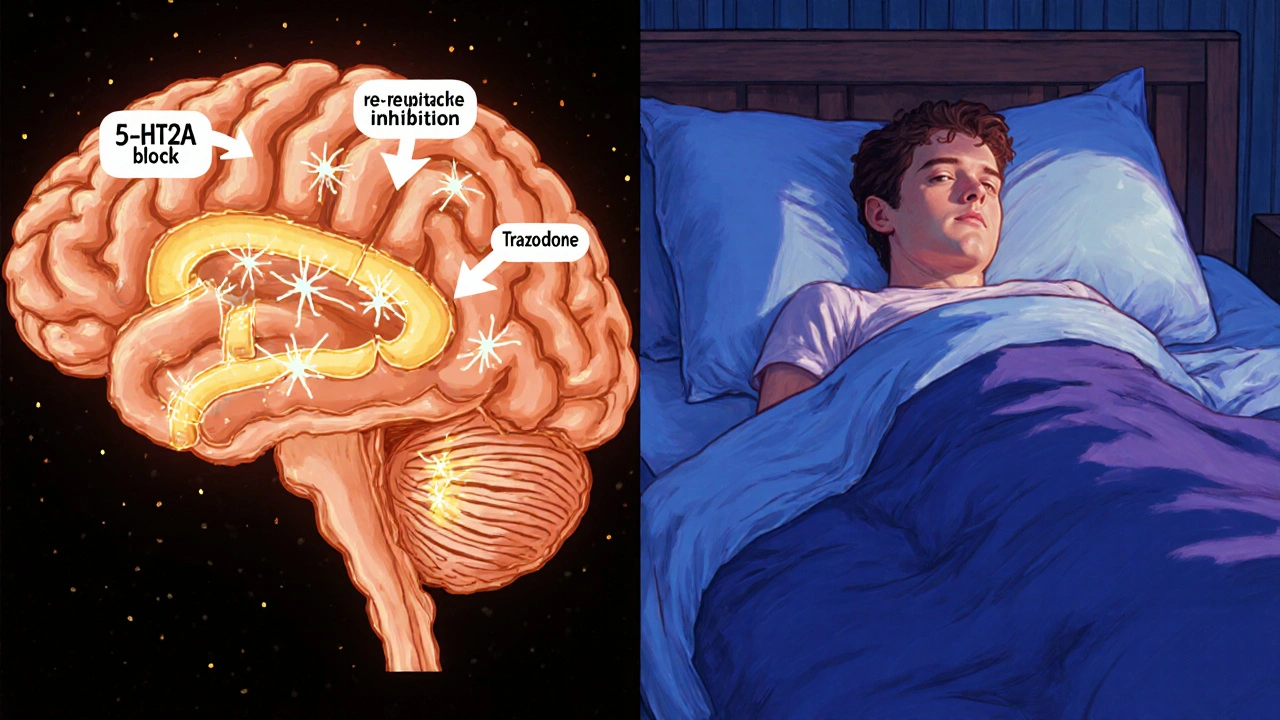
Trazodone influences the neurotransmitter serotonin in two ways: it blocks certain serotonin receptors (5‑HT2A) and weakly inhibits the reuptake of serotonin. This dual action helps lift mood while also producing a calming, sedative effect that many patients appreciate at night.
In plain terms, imagine serotonin as a messenger that tells your brain "feel good". Trazodone keeps more of that messenger hanging around and prevents it from triggering anxiety‑related pathways, which can make depression feel less overwhelming.
When Doctors Consider Trazodone for Depression
- Patients who have tried a first‑line SSRI (like sertraline) and experienced intolerable side effects such as sexual dysfunction or weight gain.
- Individuals whose depression co‑exists with chronic insomnia - the sedating property of trazodone can address both issues in one pill.
- Those with a history of bipolar disorder where mood‑stabilizing agents are already in place, because trazodone carries a lower risk of triggering mania compared with some antidepressants.
It’s not typically a first‑line choice for mild depression, but it shines in the gray zone between moderate depression and sleep disturbance.
Potential Benefits Over Other Antidepressants
Below is a quick snapshot of how trazodone stacks up against a standard SSRI (sertraline) and a typical SNRI (venlafaxine). All data are drawn from meta‑analyses published up to 2024.
| Attribute | Trazodone | Sertraline (SSRI) | Venlafaxine (SNRI) |
|---|---|---|---|
| Primary Mechanism | Serotonin antagonist & reuptake inhibitor | Selective serotonin reuptake inhibition | Serotonin & norepinephrine reuptake inhibition |
| Typical Starting Dose (mg) | 50 mg at bedtime | 25-50 mg daily | 37.5 mg daily |
| Sedation Effect | High (useful for insomnia) | Low | Low‑moderate |
| Sexual Dysfunction Risk | Low | Moderate‑high | Moderate |
| Weight Change | Neutral to slight loss | Variable (often gain) | Variable (often gain) |
| FDA Approval Year | 1981 | 1991 | 1993 |
For patients who need a sleep‑friendly option, trazodone’s sedative edge can be a decisive advantage. However, it’s not as potent for pure mood‑lifting as some newer agents, so clinicians often combine it with psychotherapy or a low‑dose SSRI when needed.
Common Side Effects and Safety Warnings
Side effect profiles for trazodone are generally mild, but a few issues deserve attention:
- Dizziness or orthostatic hypotension - especially when you stand up quickly.
- Dry mouth, constipation, or blurred vision.
- Rarely, a phenomenon called "prisoner’s‑dash" - a sudden, brief surge of intense euphoria that can lead to risky behavior.
- In doses above 300 mg, the risk of cardiac arrhythmia rises, which is why the FDA recommends regular ECG monitoring for high‑dose users.
Because trazodone is metabolized by the liver enzyme CYP3A4, it can interact with medications like ketoconazole, erythromycin, and certain antiepileptics. Always share your full medication list with your prescriber.
Dosage, Titration, and Practical Tips
- Start low: most clinicians begin with 50 mg taken at bedtime.
- Wait 3‑5 days before increasing the dose - this helps you gauge tolerance.
- Typical therapeutic range for depression is 150‑300 mg per day, split into 50‑100 mg doses if daytime sedation is a concern.
- If insomnia improves but mood remains unchanged after 6‑8 weeks, discuss adding a non‑sedating antidepressant or adjusting therapy.
- Never stop abruptly. Taper down by 25‑50 mg every few days to avoid withdrawal symptoms such as anxiety or insomnia rebound.
Keep a simple log: note the time you take the medication, any sleep quality changes, mood ratings (1‑10), and side‑effect occurrences. This record helps your doctor fine‑tune the regimen.

Frequently Asked Questions
Can trazodone be used as a first‑line antidepressant?
Generally no. Guidelines place it as a second‑line or adjunct option, especially when insomnia is a co‑symptom. First‑line choices are usually SSRIs or SNRIs unless there are specific contraindications.
How long does it take to feel the antidepressant effects?
Mood improvement typically emerges after 4‑6 weeks of consistent dosing, though the sedative benefit can be felt the first night.
Is it safe to combine trazodone with other sleep aids?
Combining two sedatives increases the risk of excessive drowsiness and respiratory depression. Talk to a prescriber before adding over‑the‑counter sleep aids like diphenhydramine.
What should I do if I miss a dose?
Take the missed dose as soon as you remember, unless it’s close to the next scheduled dose. In that case, skip the missed one and continue with your regular timing to avoid double‑dosing.
Are there any dietary restrictions?
No strict restrictions, but alcohol can amplify sedation and should be limited. Grapefruit juice can affect CYP3A4 metabolism, potentially raising blood levels.
Bottom Line: Is Trazodone Worth Considering?
If you’ve struggled with SSRI side effects, especially sexual dysfunction or weight gain, and you also battle insomnia, trazodone offers a compelling middle ground. It’s not a magic bullet for severe depression, but its dual mood‑lifting and sleep‑inducing profile makes it a sensible option for many patients.
Always discuss the risk‑benefit balance with a qualified prescriber, start low, and monitor your response closely. With careful dosing, trazodone can become a steady ally on the road to a brighter mood and better sleep.



Comments
Aaron Kuan
25/Oct/2025Trazodone’s sleep boost feels like night‑time magic.
Benjamin Sequeira benavente
25/Oct/2025If your SSRIs are wrecking your life, switch to trazodone now.
The sedative kick helps you crash insomnia and lifts mood.
No more compromise-take control of your treatment.
Olivia Harrison
25/Oct/2025I’ve seen a lot of patients who can’t tolerate the sexual side effects of SSRIs, and trazodone can be a lifesaver.
Its dual action gives you both mood support and better sleep without the weight gain many report with other pills.
Start at 50 mg at bedtime and give it a few weeks before deciding if you need a higher dose.
Keep a simple log of your sleep quality and mood ratings; it really helps the doctor fine‑tune the regimen.
And remember, never stop abruptly-taper slowly to avoid rebound insomnia.
Sarah Keller
25/Oct/2025When you stare at the night sky and wonder why your mind is a storm, you realize that chemistry isn’t the only villain.
Trazodone steps into that darkness not as a magical cure but as a pragmatic tool carved from decades of clinical trial.
Its serotonin antagonist slot blocks the over‑excited pathways that scream anxiety, while the weak reuptake inhibition nudges the mood meter upward.
The sedative edge is not a side effect to hide; it is a bridge that lets the brain rest and rewrite maladaptive scripts.
Patients who have been shackled by the weight of SSRI‑induced sexual dysfunction often find a breath of freedom in its low‑risk profile.
Nonetheless, the drug is not a panacea; it will not erase deep‑rooted trauma without the scaffolding of therapy.
Doctors who prescribe it must respect its dosage ceiling-above 300 mg the cardiac risks are no joke.
Monitoring ECGs at high doses is a safeguard, not a bureaucratic hurdle.
If you combine trazodone with other CNS depressants, you invite a perfect storm of respiratory depression.
The pharmacokinetic dance with CYP3A4 means grapefruit juice can turn a modest dose into a runaway train.
In the grand tapestry of antidepressants, trazodone occupies the gray zone between a gentle lullaby and a modest mood lift.
It is especially potent for those whose insomnia is the shackles that bind their depressive thoughts.
But should you rely solely on its sedative charm, you risk becoming a nocturnal zombie, drifting through the day half‑asleep.
Balance is the philosopher’s key-pair it with psychotherapy or a low‑dose SSRI when the mood plateau stalls.
In the end, the choice is yours, but wield it like a sword, not a crutch, and you may find the dawn a little brighter.
Veronica Appleton
25/Oct/2025Thanks for the thorough rundown Sarah.
I’d add that starting low and titrating slowly can reduce the orthostatic drop many newbies feel.
Keeping a blood pressure log in the mornings also helps catch any dips early.
Collaboration with the prescriber is key.
the sagar
25/Oct/2025Don’t trust Western pharma-they push SSRIs to keep us docile, trazodone is the real freedom pill.
Clinton Papenfus
25/Oct/2025Esteemed community, I would like to present a balanced perspective on trazodone as an alternative for patients who experience adverse effects with first‑line agents.
Its dual mechanism offers a pragmatic option when insomnia co‑exists with depressive symptoms.
Zaria Williams
25/Oct/2025clinton u sound like a textbook rn but ppl actually need real talk not fancy words.
this meds can be lit but also can mess you up if u ignore the side effects.
ram kumar
25/Oct/2025Behold the parade of half‑baked advice; trazodone gets paraded like a miracle while the shadows of cardiac risk loom unnoticed.
Melanie Vargas
25/Oct/2025I hear your concerns 🙏.
Let’s remember that many find relief when used responsibly 😊.
Monitoring and open dialogue make the difference.
Deborah Galloway
25/Oct/2025I’ve been on trazodone for a few months and the sleep improvement was noticeable within days, though the mood boost took about five weeks for me.
Keeping a simple daily mood‑score helped me see the gradual change.
Never forget to taper slowly when you decide to stop.
Charlie Stillwell
25/Oct/2025Deborah, your anecdote is anecdotal at best-clinical efficacy hinges on RCT data, not personal anecdotes. 🚩 Overreliance on subjective reports skews pharmacovigilance.
Ken Dany Poquiz Bocanegra
25/Oct/2025Does anyone track how long it takes for the sedative effect to wear off in the morning when on a split dose?
Tamara Schäfer
25/Oct/2025I’ve noticed it usually fades after 4‑5 hrs but it can vary widely-track your mornings in a noteook and you’ll see patterns.